
Photo: Freepik/diana.grytsku
Expert Profile
Vladimir Nikolaevich Plokhov, MD, PhD — Surgical Oncologist, Breast Surgeon, Dermatologic Oncologist, Professor, Doctor of Medical Sciences. Member of European Association of Dermato Oncology (EADO), European Society for Medical Oncology (ESMO), American Society of Clinical Oncology (ASCO), European Society of Endocrinology. 
Education and Board Certifications
1989 — V.I. Razumovsky Saratov State Medical University.
1991 — Surgical Residency, A.S. Loginov Moscow Clinical Scientific-Practical Center.
2019 — Advanced Training in Surgery, A.S. Loginov Moscow Clinical Scientific-Practical Center.
2019 — Advanced Training in Oncology, A.S. Loginov Moscow Clinical Scientific-Practical Center.
2020 — Advanced Training in Ultrasound Diagnostics, Interregional Center for Continuing Medical and Pharmaceutical Education.
2020 — Advanced Training in Healthcare Organization and Public Health, MEDSI Group.
2024 — Advanced Training in Oncology, A.S. Loginov Moscow Clinical Scientific-Practical Center.
2024 — Advanced Training in Surgery, A.S. Loginov Moscow Clinical Scientific-Practical Center.
2025 — Advanced Training in Ultrasound Diagnostics, Volga Regional Training Center.
Professional Experience
Over 36 years in surgical practice.
1991-1997 — Surgeon, Surgical Department, RZhD-Medicine, Saratov.
1997-2006 — Chief, Department of Oncology, RZhD-Medicine, Saratov.
2006-2012 — Medical Director, Departmental Clinical Hospital at Volgograd-1 Station, Russian Railways.
2012-2014 — Chief Medical Officer, N.A. Semashko Railway Clinical Hospital.
2014-2016 — Chief, Healthcare Department, Russian Railways.
2015-2016 — Professor, Department of Occupational Medicine, RMAPO.
2017-2018 — Surgeon, Oncologist, Breast Surgeon, Vesta-Clinic LLC.
2018-present — Chief, Department of Breast and Skin Tumors with Endocrine Surgery Center, MEDSI Clinical Hospital No. 2, Botkinsky Proyezd.
Clinical Focus: Diagnosis, prevention, and surgical treatment of benign and malignant neoplasms.
Surgical Expertise
- Sentinel lymph node biopsy for melanoma utilizing radioisotope method;
- sentinel lymph node biopsy for breast cancer utilizing fluorescent and radioisotope methods;
- endoscopic thyroid procedures;
- breast-conserving surgery for malignant and benign tumors;
- prophylactic mastectomy for genetic mutations;
- lymph node dissection for breast cancer metastases;
- total thyroidectomy with central lymph node dissection;
- hemithyroidectomy with isthmusectomy; recurrent laryngeal nerve neurolysis for involvement in tumor process in thyroid malignancy;
- melanoma excision with reconstructive surgical component; inguinal-femoral and axillary lymph node dissections for melanoma metastases; oncologic resection with reconstructive surgery for basal cell and squamous cell carcinoma;
- soft tissue sarcoma resection of any anatomic location;
- procedures for non-palpable breast and soft tissue tumors with wire localization under ultrasound guidance;
- procedures for intraductal breast papillomas with intraoperative duct localization;
- interventional diagnostic procedures: core needle biopsy of breast lesions under ultrasound guidance, core needle biopsy of lymph nodes under ultrasound guidance, core needle biopsy of soft tissue neoplasms under ultrasound guidance, thyroid fine needle aspiration;
- reconstructive surgery: immediate and delayed breast reconstruction with implants or autologous tissues, microsurgical DIEP flap; augmentation mammoplasty (breast enlargement and reshaping) using silicone implants or autologous tissues;
- autologous fat grafting (breast augmentation using fat transfer); reduction mammoplasty (breast reduction);
- mastopexy (breast lift); liposuction; blepharoplasty; abdominoplasty.
The Clinical Consequences of Delayed Presentation in Cutaneous Malignancy
Basal cell carcinoma is the most common form of non-melanoma skin cancer. With timely presentation, radical tumor resection with minimal aesthetic defects is typically achievable, preserving both function and appearance of the affected anatomic site.
Unfortunately, advanced presentations remain common where the tumor has extensively invaded beyond the epidermis and involves underlying structures—muscle, cartilage, and bone. Such advanced cases are most frequently associated with patient fear of medical consultation and surgical intervention, and occasionally with delayed access to specialized oncologic care. Consequently, instead of a minor planned procedure, a complex oncologic problem must be addressed with significant functional and aesthetic consequences for the patient.
Basal cell carcinoma is a cutaneous malignancy that develops from the basal layer of the epidermis. This malignant neoplasm most frequently appears on sun-exposed anatomic sites—face, nose, ears, neck—and typically demonstrates slow growth, rarely metastasizes, but can deeply invade tissues, destroying skin, cartilage, and bone if left untreated for extended periods.
Four Years Without Medical Consultation
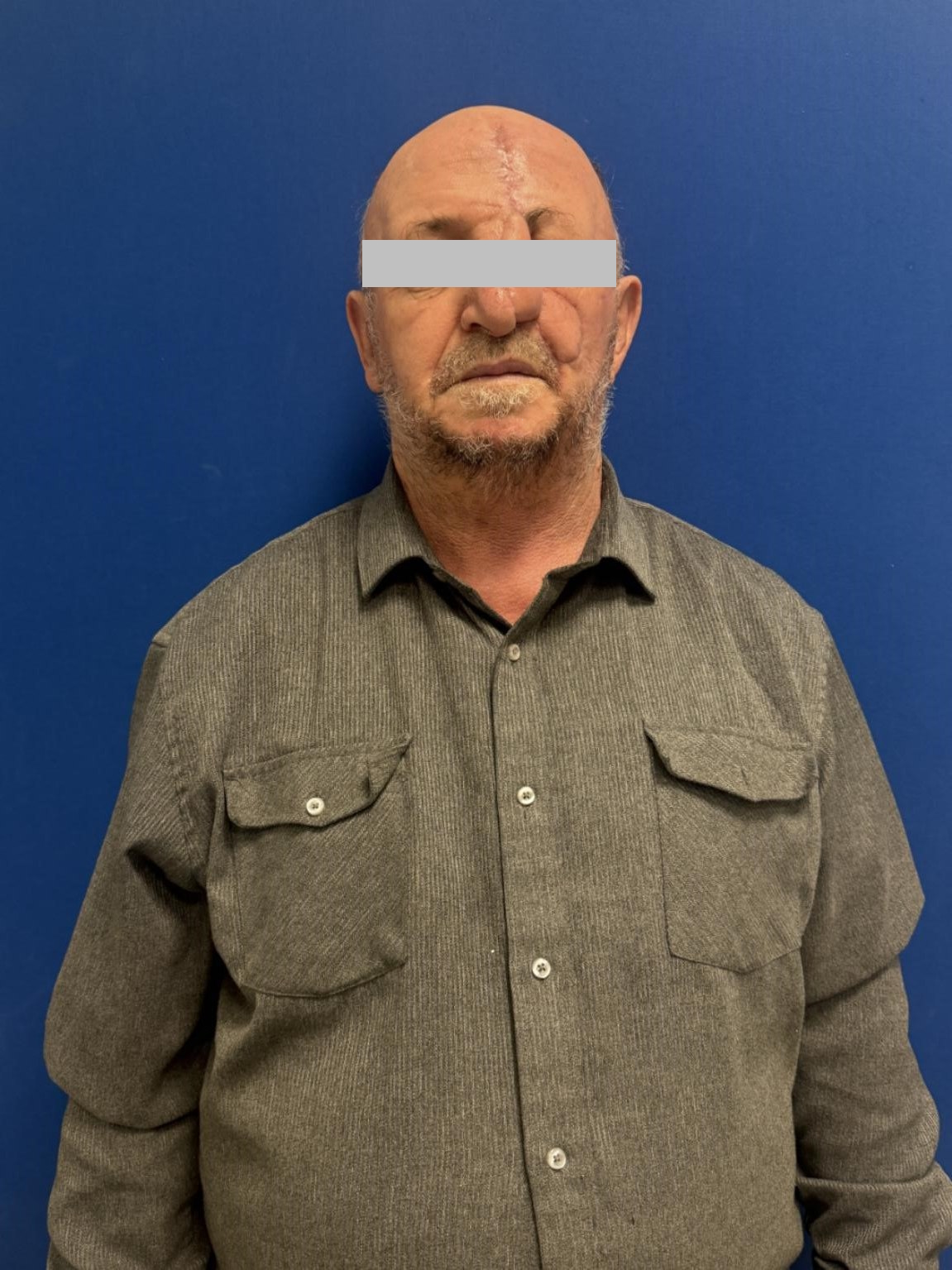
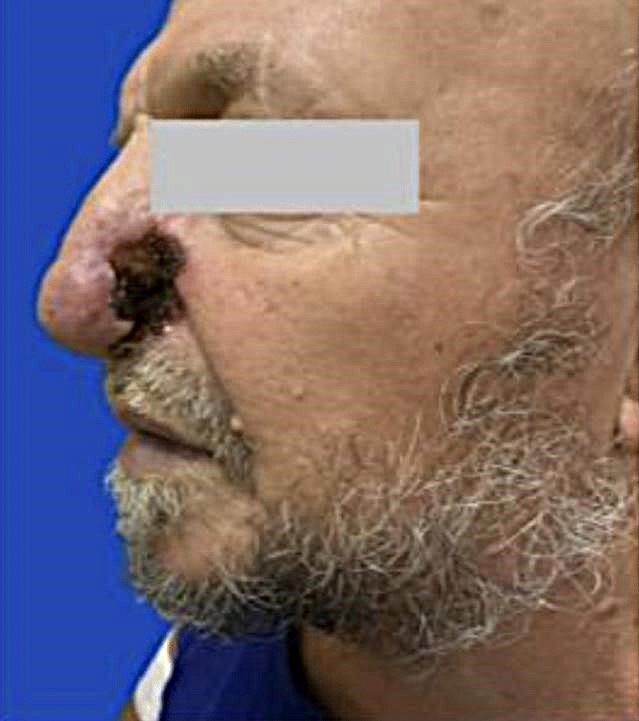
Patient N, a 68-year-old male, in 2021 noted the appearance of a small ulcerative defect on the left nasal ala but did not seek medical attention, attributing it to accidental trauma while playing with his grandson. Over time, he independently initiated topical treatment with various ointments; however, despite these interventions, the ulceration failed to heal and progressively increased in size, involving an expanding area of surrounding skin.
By 2025, the tumor occupied practically the entire left nasal ala with complete destruction of skin and underlying cartilage, extending to the nasal dorsum and left malar region. To continue interacting with grandchildren and family members, the patient was required to wear a nasal prosthesis to avoid distressing others. Intermittently he noted bleeding at the ulcer margins during facial washing and any contact with the affected area.
At the time of presentation to local specialists, the patient had developed an ulcerative defect approximately 4 cm with near-complete destruction of the left nasal ala. In February 2025, tissue biopsy of the nasal lesion was performed with histopathologic confirmation of basal cell carcinoma. Radiation therapy was recommended by local providers; however, treatment was never initiated.
Clinical Evaluation and Organ-Preservation Surgical Planning
In September 2025, the patient presented to MEDSI clinic where comprehensive diagnostic evaluation was performed.
Magnetic resonance imaging (MRI) of facial soft tissues revealed a pathologically altered cutaneous area measuring approximately 11×4×15 mm in the left nasal ala region with pronounced contrast enhancement, closely approximating the lower lateral cartilage without definitive signs of cartilaginous invasion. Within the left nasal cavity, parietal mucosal edema was identified, extending to tumor level for approximately 17 mm and demonstrating contrast uptake.
Computed tomography (CT) of facial skeleton soft tissues revealed no evidence of osseous involvement at this level, suggesting feasibility of organ-preservation surgery with limited resection margins.
Surgical Strategy: Mohs Micrographic Surgery and Flap Reconstruction
The patient underwent rhinoscopy, which excluded nasal cavity involvement in the tumor process.
Based on imaging studies and clinical examination, surgical intervention was planned: nasal cutaneous tumor excision with adequate tissue margins utilizing Mohs micrographic technique with intraoperative frozen section histologic assessment, with simultaneous defect closure using transposition flap reconstruction.
This methodology allows maximal precision in determining whether tumor cells remain at resection margins: macroscopically the skin may appear normal, yet micrographic examination can reveal occult tumor extension and provides the opportunity to immediately excise involved areas.
Intraoperatively, all resection margins were evaluated: the tumor was resected with clear margins, with no evidence of residual tumor cells at any margin. Following complete resection, a defect measuring 5.5 × 6.0 cm remained.
Subsequently, reconstructive surgery was performed: utilizing a combination of cheek and forehead flaps based on vascular pedicles, the defect was closed and the left nasal structure was simultaneously reconstructed, preserving anatomic contour and volume.
Clinical Outcome: Restored Function and Social Reintegration
The patient was discharged in stable condition on postoperative day 2; the postoperative course and recovery proceeded without complications.
At follow-up examination, no nasal airway obstruction was noted. The patient reported not only physical comfort but also marked improvement in social engagement: he resumed normal interaction with family members and playing with grandchildren without need to conceal the facial defect.
Timely medical consultation for any cutaneous changes or physical symptoms, even those initially appearing trivial or attributable to minor trauma, is critical.
This patient's case clearly demonstrates that a "benign-appearing" abrasion or chronic non-healing cutaneous wound can represent the initial presentation of a serious oncologic process if neglected for months or years.
Regular medical examinations and prompt physician consultation for any new lesions, ulcerations, indurations, or pigmentary changes is not excessive vigilance but rather a strategy to detect malignancy at a stage when it can be resected with minor surgery, without complex reconstruction and significant impact on appearance and quality of life.
See the results of the operation in the photo gallery
All information on this website is provided for informational purposes only and does not constitute medical advice. All medical procedures require prior consultation with a licensed physician. Treatment outcomes may vary depending on individual characteristics. We do not guarantee any specific results. Always consult a medical professional before making any healthcare decisions.